1Institute of Endocrinology, University Clinical Center, Belgrade, Yugoslavia, 2Department of Physiology and 3Department of Medicine, Faculty of Medicine, University of Santiago de Compostela, Santiago de Compostela, Spain
The aim of this study was to evaluate the influence of circulating cortisol levels on the somatotroph responsiveness to the most potent stimuli of growth hormone (GH) secretion, the GHRH+GHRP-6 test. We studied 12 patients with hypocortisolism (10 with Addison's disease and 2 with isolated ACTH deficiency) before and after glucocorticoid (GC) replacement therapy and compared them with 14 healthy subjects. In the 10 patients with Addison's disease, GH responses (GH peak, µg/L) to GHRH+GHRP-6 were similar both during GC, (68.2±12.8) and off GC (60.3±14.1) therapy and did not differ from those in controls (61.5±6.0). In a subgroup of 4 patients with newly diagnosed Addison's disease, GH responsiveness to GHRH+GHRP-6 prior to GC replacement (26.4±4.1) was significantly lower than in the 6 patients with long-standing Addison's disease after short-term GC withdrawal (82.9±18.2). In the newly diagnosed Addison's patients, after one month of GC replacement, mean GH peak value increased to 40.7±11.8. In the 2 patients with isolated ACTH deficiency, GH responses to GHRH+GHRP-6 did not differ off and on GC therapy (60.3±14.1 and 41.5±2.0, respectively). Our data suggest that short-term GC deprivation does not have a major impact on GH responsiveness to GHRH+GHRP-6. However, in patients with long-standing hypocortisolism, GH response is blunted but still within normal range (> 15 µg/L).
Growth hormone, hypocortisolism, GHRH+GHRP-6
INTRODUCTION
Endogenous glucocorticoids play an important physiological role in the regulation of somatotroph function1. These steroids regulate growth hormone (GH) synthesis and secretion by modulating both hypothalamic and pituitary function2. Chronic glucocorticoid excess causes growth retardation and inhibits GH secretion and GH responsiveness to several stimuli, including GHRH and GHRP-63-8. The precise mechanisms by which this occurs are unknown. Glucocorticoids inhibit GHRH and/or stimulate somatostatin synthesis and release9,10,11. At the pituitary level, glucocorticoids increase the GH and GH-releasing hormone receptor (GHRH-R) and pituitary GH secretagogue receptor (GHS-R) synthesis and gene expression and enhance the stability of GH mRNA12-16. Therefore, physiological amounts of glucocorticoids are important for the hypothalamic-pituitary somatotroph axis.
The effect of glucocorticoid deprivation on GH release has been less extensively studied in both animals and man. In rats, adrenalectomy decreases GH responsiveness to GHRH, whereas glucocorticoid treatment has the opposite effect, probably as a result of a decrease in GHRH receptor number and changes in pituitary sensitivity to GHRH17,18. Patients with ACTH deficiency and prolonged hypocortisolism also have reduced GH responsiveness to several stimuli, including GHRH19,20. Studies on the effects of short-term hypocortisolism on GH secretion in man are conflicting. In normal subjects pretreated with metyrapone and in patients with Addison's disease, an acute decrease in circulating cortisol level does not alter GH responsiveness to GHRH or GHRP-621,22. An increase in GHRH-induced GH release in normal subjects was found by lowering cortisol levels23,24.
GH-releasing peptide-6 (GHRP-6) is a synthetic hexapeptide that releases GH through GHS-R by a mechanism which differs from that of GHRH25-27. This hexapeptide activates hypothalamic and pituitary GHS-R whose natural ligand, ghrelin, was recently discovered28-30. We demonstrated that the combined administration of GHRH + GHRP-6 is a useful test
of GH reserve in adult patients and may become the new gold standard test in a variety of clinical settings, particularly in the evaluation of adults suspected of growth hormone deficiency31-34.
The aim of the present study was to investigate the possible influence of serum cortisol levels on GH response to the combined GHRH+GHRP-6 test in adult patients with primary and secondary adrenal insufficiency, in which we do not expect GH deficiency. Specifically, there were patients without clinical symptoms or signs of GH deficiency, and without organic pathology in the hypothalamic/pituitary region.
SUBJECTS AND METHODS
Subjects
1. Addison's disease
Ten patients with autoimmune Addison's disease (1 man and 9 women) were studied (Tables 1 and 2 ). Their mean age was 43.1 ± 4.2 yrs (range 22 - 68) and the mean body mass index (BMI) was 22.5 ± 1.2 kg/m2 (range 16.7 - 30.0). Six patients had long-standing hypocortisolism and had been receiving glucocorticoid replacement therapy with hydrocortisone acetate for more than two years (Table 1), while 4 patients had newly diagnosed Addison's disease (Table 2 ). Hydrocortisone was administered at a dose of 30 µg/day, divided into 2 doses (at 0800 and 1600 h). Five patients also had mineralocorticoid deficiency and received replacement therapy with fludrocortisone at a dose of 0.1 µg/day. One patient with Addison's disease (patient 4, Table 2) also had associated premature ovarian insufficiency and primary hypothyroidism and was receiving adequate replacement therapy with L-thyroxine at doses of 100 µg/day.
The results obtained in the patients were compared with those of a control group consisting of 14 healthy female subjects (age 40.4 ± 3.2 yrs, range 22 - 64 yrs; BMI 23.2 ± 0.8 kg/m2, range 18.1 - 30.3). They were free of any medication at the time of the study. The women were tested in the early follicular phase of their menstrual cycles.
2. Isolated ACTH deficiency
Two patients with newly diagnosed isolated ACTH deficiency (both women) were studied. Their mean age was 46.0 ± 5.0 yrs and mean BMI was 21.6 ± 1.1 kg/m2.
Study protocol
The GHRH+GHRP-6 test was performed after an overnight fast, and the subjects remained recumbent throughout. One hour before starting the test (0800h), an indwelling catheter was inserted into an antecubital vein and was kept patent by a slow saline infusion. After 3 basal blood samples (-30, -15 and 0 minutes), all subjects received GHRH (1 µg/kg, GRF 1-29 NH2, Geref Serono, Madrid, Spain) + GHRP-6 (1 µg/kg, His-D-Trp-Ala-Trp-D-Phe-Lys-NH2; Clinalfa Laufelfinger, Switzerland). Blood samples were subsequently obtained at 15, 30, 45, 60, 90 and 120 minutes for GH measurements. Normal growth hormone response to GHRH+GHRP-6 was previously defined as a peak GH concentration greater than 15 µg/L32. Serum cortisol level was measured at baseline on and off glucocorticoid therapy.
Adrenal insufficiency. Six patients with long-standing Addison's disease were studied on two occasions, with an interval of at least 30 days between the tests. On the first occasion, they received GHRH+GHRP-6 during their regular hydrocortisone replacement therapy on an out-patient basis. To avoid a possible stimulating effect of acute glucocorticoid administration on GHRH+GHRP-6 induced GH release, on the morning of the test the patients received their dose of hydrocortisone after the test. The second GHRH+ GHRP-6 test was performed after 72h withdrawal of hydrocortisone therapy, and the patients were hospitalized. All patients developed clinical signs of adrenal insufficiency during hydrocortisone withdrawal.
Four patients who had newly diagnosed Addison's disease were studied on two occasions: before hydrocortisone replacement and after one month of hydrocortisone therapy.
Isolated ACTH deficiency. Two patients who had newly diagnosed isolated ACTH deficiency were studied twice with GHRH+GHRP-6 test: before hydrocortisone replacement and after one month of hydrocortisone therapy (30 µg/day in two doses).
Each control subject underwent the GHRH+ GHRP-6 test as described above. The local ethical committee approved the protocol and all the subjects gave informed consent.
Methods
Serum GH was measured with a time-resolved fluoroimmunoassay (Wallac, Turcu, Finland, µg/L) with sensitivity of assay 0.011 µg/L and with CV 6.3% (0.4 µg/L), 5.3% (10.2 µg/L), 4.2% (43.4 µg/L). Serum cortisol was measured with a radioimmunoassay (RIA, INEP, Zemun, nmol/L) with CV 16.6% (115 nmol/L), 2.5% (584 nmol/L), 5.9% (1001 nmol/L).
Statistical analysis
Results are reported as the mean ± SE. Growth hormone responses to the combined test were quantified by determining the area under the curve (AUC), calculated using trapezoidal integration. Data were analysed using non-parametric methods including the Mann-Whitney rank sum test for independent samples and the Wilcoxon rank test for data.
RESULTS
1. Addison's disease
In all patients with Addison's disease, GH responses to GHRH+GHRP-6 were similar both during standard replacement therapy (GH peak, 68.2 ± 12.8 µg/L; AUC, 3601 ± 694 µg/L/120min) and without hydrocortisone (GH peak, 60.3 ± 14.1 µg/L; AUC, 3201 ± 692 µg/L/120min, p > 0.05) and did not differ from those in controls (GH peak, 61.5 ± 6.0 µg/L; AUC, 3500 ± 413 µg/L/120min, p > 0.05). In the six patients with long-standing Addison's disease, a similar GH response after the GHRH+GHRP-6 test was seen both during replacement therapy (GH peak, 86.5 ± 16.4 µg/L; AUC, 4721 ± 768 µg/L/120min) and after short-term glucocorticoid withdrawal (GH peak, 82.9 ± 18.2 µg/L; AUC, 4336 ± 863 µg/L/120min, p > 0.05; Figures 1a and 1b). Moreover, the patients with long-standing Addison's disease both on and off replacement therapy did not show significant changes in GH release compared to the normal subjects (GH peak, 61.5 ± 6.0 µg/L; AUC, 3500 ± 413 µg/L/120min, p > 0.05). All the patients had peak GH values above 15 µg/L on and off replacement therapy. As expected, hydrocortisone withdrawal was associated with a decrease in circulating cortisol (962.0 ± 117.0 nmol/L vs. 23.9 ± 12.3 nmol/L; p < 0.05). In our group of patients, glucocorticoid withdrawal for 72h caused clinical signs of adrenal insufficiency, but all manifestations were well tolerated. None of the patients had to interrupt the study protocol.
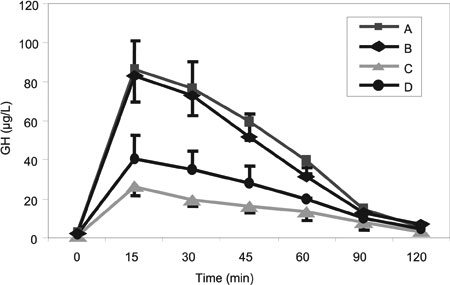
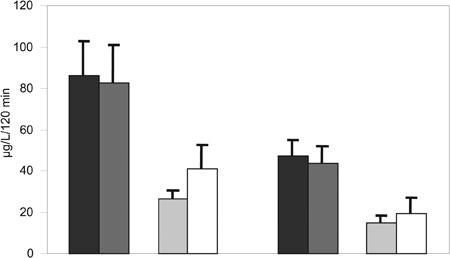
Figure 1. Mean plasma GH levels (a: mean peak ± SE, b: mean peak and mean area under the curve ± SE) after GHRH+GHRP-6 administration in: A - Patients with long-standing Addison's disease on hydrocortisone therapy; B - Patients with long-standing Addison's disease 72h off hydrocortisone therapy; C - Patients with newly diagnosed Addison's disease before hydrocortisone therapy; D - Patients with newly diagnosed Addison's disease after one month of hydrocortisone therapy.
** C vs. B p < 0.01
In the 4 patients with newly diagnosed Addison's disease, GH responsiveness to GHRH+GHRP-6 before hydrocortisone replacement was significantly lower in comparison with patients in whom hydrocortisone was acutely withdrawn (GH peak, 26.4 ± 4.1 µg/L vs. 82.9 ± 18.2 µg/L, p < 0.01; AUC, 1498 ± 335 µg/L/120min vs. 4336 ± 863 µg/L/120min, p < 0.01; Figures 1a and 1b). No differences in age and BMI were seen between the two groups. GH response to the GHRH+GHRP-6 test increased after one month of replacement therapy with hydrocortisone (GH peak, 40.7 ± 11.8 µg/L; AUC, 1920 ± 756 µg/L/120min), statistically not different from the patients with long-standing Addison's disease on standard hydrocortisone therapy (GH peak, 86.5 ± 16.4 µg/L; AUC, 4721 ± 768 µg/L/120min, p = 0.088; Figures 1a and 1b). Serum cortisol levels at the time of diagnosis were 20.8 ± 3.8 nmol/l, increasing after one month of stable hydrocortisone replacement therapy (613.0 ± 60.0 nmol/L; p < 0.05).
2. Isolated ACTH deficiency
In the two patients with newly diagnosed isolated ACTH deficiency, GH responsiveness to GHRH+ GHRP-6 were similar both before hydrocortisone therapy (GH peak, 64.9 ± 4.6 µg/L) and while on hydrocortisone (GH peak, 41.5 ± 2.0 µg/L; p > 0.05) and did not differ from those in controls (GH peak, 61.5 ± 6.0 µg/L; p > 0.05).
DISCUSSION
The aim of the present study was to investigate whether the GH response to the most potent GH stimuli, the combined GHRH+GHRP-6 test is affected by low serum cortisol levels in two groups of patients in whom we did not suspect GH deficiency. Patients with primary adrenal insufficiency and those with isolated ACTH deficiency served as a model for the investigation of the influence of serum cortisol levels on GH responsiveness to the provocative stimuli.
In the patients with Addison's disease on stable replacement therapy, GH responsiveness to the GHRH+GHRP-6 test was normal. In these patients, an acute decrease in circulating cortisol levels, caused by 72h-withdrawal of hydrocortisone, did not significantly modify the GH response to GHRH+GHRP-6. GH responses to GHRH+GHRP-6 both with and without hydrocortisone therapy were similar to and not different from the control subjects.
The patients with newly diagnosed Addison's disease (i.e. prolonged glucocorticoid deprivation), who were chronically severely depleted of glucocorticoids, had a blunted GH response to GHRH+GHRP-6, but still within the normal range (a GH response over 15 µg/L), indicating subtle changes in somatotroph function. After one month of glucocorticoid replacement therapy, GH response to the GHRH+GHRP-6 test increased, suggesting the possibility of transitory reduction of GH secretion, possibly caused by low cortisol levels.
Our data are in agreement with the results of Pin
to et al, demonstrating that somatotroph function is preserved in states of acute glucocorticoid deprivation21. In their study, an acute decrease in circulating cortisol levels, achieved with metyrapone pretreatment, did not change the GH response to GHRP-6 in normal subjects. Patients with chronic hypoadrenalism on hydrocortisone therapy had normal increase in GH levels after GHRP-6, and after glucocorticoid interruption for 72h, no significant change in GH responsiveness was observed. They concluded that short-term glucocorticoid deprivation does not have a major impact on GHRP-6-dependent GH release.
In patients with ACTH deficiency, prolonged glucocorticoid deprivation reduced GH responsiveness to several stimuli, including insulin- induced hypoglycemia, arginine and GHRH19,20 and glucocorticoid replacement therapy restored GH release after GHRH administration19,20. The authors concluded that in patients with idiopathic ACTH deficiency, an impaired GH response to stimuli, reversible during glucocorticoid replacement therapy, may be the consequence of the low cortisol levels. These patients were studied with an insulin tolerance test and an arginine infusion test, which are less potent GH releasers than the combined GHRH+GHRP-6 test. In our two patients with isolated ACTH deficiency, GH response to the GHRH+GHRP-6 test was normal before and after one month of hydrocortisone therapy. These data are in agreement with the results of Sakai et al, who demonstrated complete ACTH deficiency after radiation therapy for brain tumor with a normal GH reserve35.
It has been shown that glucocorticoids have a stimulatory effect on pituitary GHRH and GHS-R synthesis, at least in the rat36—38. Adrenalectomy markedly decreases GHS-R gene expression, whereas glucocorticoid treatment has the opposite effect36,37. It is possible that in Addison's patients with prolonged hypocortisolism before glucocorticoid replacement, GHRH-R and GHS-R are down-regulated with consequent attenuation of GHRH+GHRP-6-induced GH release. It is likely that in these hypoadrenal patients, even after adequate glucocorticoid replacement therapy, circulating glucocorticoid levels are inadequate to maintain a completely normal pituitary GHRH-R and GHS-R synthesis and somatotroph function.
In conclusion, our data suggest that short-term glucocorticoid deprivation does not modify the GH responsiveness to GHRH+GHRP-6. However, in long- standing hypocortisolism, GH response to the combined test is blunted, yet still within the normal range, suggesting the presence of subtle changes in somatotroph function.
REFERENCES
1. Devesa J, Lima L, Tresguerres LAF, 1992 Neuroendocrine control of growth hormone secretion in humans. Trends Endocrinol Metab 3: 175-183.
2. Thakore JH, Dinan TG, 1994 Growth hormone secretion: the role of glucocorticoids. Life Sci 55: 1083-1099.
3. Magiakou MA, Mastorakos G, Gomez MT, Rose SR, Chrousos GP, 1984 Suppressed spontaneous and stimulated growth hormone secretion in patients with Cushing's disease before and after surgical cure. J Clin Endocrinol Metab 78: 131-137.
4. Hotta M, Shibasaki T, Masuda A, et al, 1988 Effect of human growth hormone-releasing hormone on GH secretion in Cushing' syndrome and nonendocrine diseases patients (O.K.?) treated with glucocorticoids. Life Sci 42: 979-984.
5. Leal-Cerro A, Pumar A, Garcia-Garcia E, Dieguez C, Casanueva FF, 1994 Inhibition of growth hormone release after the combined administration of GHRH and GHRP-6 in patients with Cushing's syndrome. Clin Endocrinol 41: 649-654.
6. Borges MH, DiNinno FB, Lengyel AM, 2002 Different effects of growth hormone releasing peptide (GHRP-6) and GH-releasing hormone on GH release in endogenous and exogenous hypercortisolism. Clin Endocrinol 46: 713-718.
7. Giustina A, Bussi AR, Deghenghi R, et al, 1995 Comparison of the effects of growth hormone-releasing hormones and hexarelin, a novel growth hormone-releasing peptide-6 analog, on growth hormone secretion in humans with or without glucocorticoid excess. J Endocrinol 146: 227-232.
8. Pinto AC, Finamor FE Jr, Lengyel AM, 1999 Acute dexamethasone administration enhances GH responsiveness to GH releasing peptide-6 (GHRP-6) in man. Clin Endocrinol 51: 409-414.
9. Takahashi H, Bando H, Zhang C, Yamasaki R, Saito S, 1992 Mechanism of impaired growth hormone secretion in patients with Cushing's syndrome. Acta Endocrinol 127: 13-17.
10. Dieguez C, Mallo F, Senaris R, et al, 1996 Role of glucocorticoids in the neuroregulation of growth hormone secretion. J Pediatr Endocrinol Metab 9: 255-260.
11. Leal-Cerro A, Pumar A, Villamil F, Astorga R, Dieguez C, Casanueva FF, 1993 Growth hormone releasing hormone priming increases growth hormone secretion in patients with Cushing's syndrome. Clin Endocrinol 38: 399-403.
12. Evans RM, Bimberg NC, Rosenfeld MG, 1992 Glucocorticoid and thyroid hormones transcriptionally regulate growth hormone gene expression. Proc Natl Acad Sci USA 79: 7659-7663.
13. Lam KSL, Lee MF, Tam SP, Srivastava GS, 1996 Gene expression of the receptor for growth hormone-releasing hormone is physiologically regulated by glucocorticoids and estrogen. Neuroendocrinology 8: 475-480.
14. Tamaki M, Sato M, Matsubara S, Wada Y, Takahara J, 1996 Dexamethasone increases growth hormone (GH)-releasing hormone (GRH) receptor mRNA levels in cultured rat anterior pituitary cells. J Neuroendocrinol 8: 475-480.
15. Paek I, Axel R, 1998 Glucocorticoids enhance stability of human growth hormone mRNA. Mol Cell Biol 77: 1496-1507.
16. Tamura H, Kamegai J, Sugihara H, Kineman RD, Frohman LA, Wakabayashi I, 2000 Glucocorticoids regulate pituitary growth hormone secretagogue receptor gene expression. J Neuroendocrinol 12: 481-485.
17. Wehrenberg WB, Baird A, Ling N, 1993 Potent interaction between glucocorticoids and growth hormone-releasing factor in vivo. Science 221: 556-557.
18. Oyhama T, Sato M, Ohye H, Murao K, Niimi M, Takahara J, 1998 Effects of adrenalectomy and glucocorticoid receptor antagonist, RU38486, on pituitary growth hormone-releasing hormone receptor gene expression in rats. Peptides 19: 1063-1067.
19. Hochberg Z, Hardoff D, Atias D, Spindel A, 1985 Isolated ACTH deficiency with transitory GH deficiency. J Endocrinol Invest 8: 67-70.
20. Giustina A, Romanelli G, Candrina R, Giustina G, 1989 Growth hormone deficiency in patients with idiopathic adrenocorticotropin deficiency resolves during glucocorticoid replacement. J Clin Endocrinol Metab 68: 120-124.
21. Pinto AC, Silva M, Martins M, Brunner E, Lengyel AM, 2000 Effects of short-term glucocorticoid deprivation on growth hormone (GH) response to GH-releasing peptide-6: studies in normal man and in patients with adrenal insufficiency. J Clin Endocrinol Metab 85: 1540-1544.
22. Giustina A, Bresciani E, Bossoni S, et al, 1994 Reciprocal relationship between the level of circulating cortisol and growth hormone secretion in response to growth hormone-releasing hormone in man: studies in patients with adrenal insufficiency. J Clin Endocrinol Metab 79: 1266-1272.
23. Burguera B, Muruais C, Penalva A, Dieguez C, Casanueva FF, 1990 Dual and selective actions of glucocorticoids upon basal and stimulated growth hormone release in man. Neuroendocrinology 51: 51-58.
24. Dinan TG, Thakore J, O'Keane V, 1994 Lowering cortisol enhances growth hormone response to growth hormone releasing hormone in healthy subjects. Acta Physiol Scand 151: 413-416.
25. Bowers CY, Momany FA, Reynolds GA, Hong A, 1984 On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone. Endocrinology 114: 1537-1545.
26. Cheng K, Chan WW, Butler B, Barreto A Jr, Smith RG, 1991 Evidence for a role of protein kinase-C in His-D-Trp-Ala-Trp-D-Phe-Lys-NH2-induced growth hormone-release from rat primary pituitary cells. Endocrinology 129: 3337-3342.
27. Howard AD, Feighner SD, Cully DF, et al, 1996 A receptor in pituitary and hypothalamus that functions in growth hormone release. Science 273: 974-977.
28. Casanueva FF, Dieguez C, 1999 Growth hormone secretagogues, physiological studies and clinical utility. Trends Endocrinol Metab 10: 30-38.
29. Kojima M, Hosoda H, Date Y, Nakazoto M, Matsuo H, Kangawa K, 1999 Ghrelin is a growth hormone-release acylated peptide from stomach. Nature 402: 656-660.
30. Bowers CY, Sartor AO, Reynolds GA, Badger TM, 1991 On the actions of the growth hormone-releasing hexapeptide, GHRP. Endocrinology 128: 2027-2035.
31. Ho KKY, 2000 Diagnosis of adult GH deficiency. Commentary. Lancet 356: 1125-1126.
32. Popovic V, Leal A, Micic D, et al, 2000 GH-releasing hormone and GH-releasing peptide-6 for diagnostic testing in GH-deficient adults. Lancet 356: 1137-1142.
33. Popovic V, Pekic S, Simic M, et al, 2002 Physical activity or food intake prior to testing did not affect the reproducibility of GH secretion elicited by GH releasing hormone plus GH-releasing hexapeptide in normal adult subjects. Clin Endocrinol 56: 89-94.
34. Leal A, Lage M, Popovic V, et al, 2002 A single growth hormone (GH) determination is sufficient for the diagnosis of GH-deficiency in adult patients using the growth hormone releasing hormone plus growth hormone releasing peptide-6 test. Clin Endocrinol 57: 377-384.
35. Sakai H, Yoshioka K, Yamagami K, et al, 2002 Complete adrenocorticotropin deficiency after radiation therapy for brain tumor with a normal growth hormone reserve. Intern Med 41: 453-457.
36. Thomas GB, Bennet PA, Carmignac DF, Robinson CAF, 1998 Glucocorticoid regulation of GH-releasing peptide-6-induced growth responses and GH secretagogue-receptor gene expression in the rat. Proc of the 80th Annual Meet of The Endocrine Soc, 229.
37. Kamegai J, Tamura H, Ishii S, et al, 1999 Glucocorticoid regulation of pituitary growth hormone secretagogue receptor (GHR-S) gene expression. Proc of the 81th Annual Meet of The Endocrine Soc, 381.
38. Ono M, Makino R, Miki N, 1999 Thyroid hormone and glucocorticoid regulation of growth hormone secretagogue and growth hormone-releasing hormone receptor gene expression. Proc of the 81th Annual Meet of The Endocrine Soc, 381.
Address correspondence and requests for reprints to:
Professor Vera Popovic, Institute of Endocrinology,
Dr Subotica 13, 11000 Belgrade, Yugoslavia,
Tel: + 381 11 3616317, Fax: + 381 11 685357,
e-mail: popver@eunet.yu
Received 16-07-03, Revised 19-08-03, Accepted 15-09-03