1Third Department of Surgery, 2Department of Endocrinology, 3Department of Gastroenterology, 4Department of Pathology, Athens General Hospital, Athens, 115 27, Greece
We report a case of an insulinoma that was not identified on either Computerized Tomography (CT) scan and Magnetic Resonance Imaging (MRI). Endoscopic ultrasonography (EUS) revealed a small insulinoma located at the body of the pancreas, which was histologically confirmed. The patient underwent a laparotomy but no tumour was identified either on palpation or with intra-operative ultrasound (IOUS). Subsequently, a further EUS was performed and after the tumour was identified was injected with blue dye. The patient then underwent a second exploratory laparotomy and a tumour at the posterior aspect of the pancreas close to the left side of the portal vein was identified and was successfully excised. Histology confirmed the presence of an endocrine tumour staining for chromogranin A and insulin. The patient had an uneventful postoperative recovery and has developed no further episodes of hypoglycemia 3 years after surgery.
Endoscopic ultrasound, Hypoglycemia, Insulinoma
INTRODUCTION
Insulinomas are rare, mostly benign endocrine tumours that can effectively be cured with surgical excision1. The majority of pancreatic insulinomas is of small size and may not be easily exposed during the surgical procedure particularly if they are not located at the anterior surface of the gland2. Traditionally, blind distal pancreatectomy had been the standard surgical procedure when a tumour could not be visualized and/or palpated intra-operatively. However, with the advance in diagnostic and localization techniques, blind resections for small and benign insulinomas have been avoided1. Preservation of the pancreatic parenchyma is currently considered mandatory as insulinomas are mainly benign tumours and most patients remain well following successful excision even after prolonged follow-up2. Pre-operative Endoscopic Ultrasonography (EUS) and Intraoperative Ultrasound (IOUS) as well as careful surgical palpation are associated with an almost 100% sensitivity in identifying eutopically (endo-pancreatic) localized small insulinomas that have eluded detection with pre-operative conventional imaging studies.
We report a case of a small pancreatic insulinoma for which we have operated on twice. In the first operation a soft tissue mass, which was in continuation with the pancreas, was removed and was proven to be a lymph node. EUS provided important aim in guiding fine needle for preoperative tattooing (FNT) of the tumour area and enucleation of the tumour was easily performed. The patient remains cured almost 3 years following the successful removal of the insulinoma.
CASE REPORT
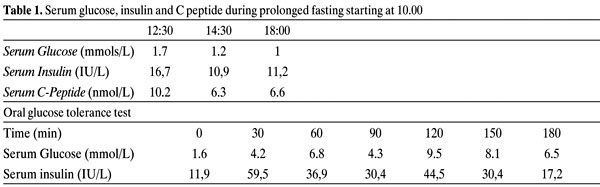
A 17-year-old female presented to the Emergency Department after an episode of loss of consciousness during the night accompanied by seizures. Her relatives gave a history of a fasting period of more than 8 hours before the initiation of her symptoms. Clinical examination revealed no neck stiffness or any other focal neurological signs. A serum glucose taken at the Emergency Department while the patient was unconcious was low and the patient was given intravenous injection of hypertonic glucose. She was admitted to the Department of Neurology for further investigation. CT scan and MRI of her brain did not demonstrate any brain lesion. However, as she remained hypoglycemic (serum glucose levels ranging from 1.6 to 3 mmol/L) a provisional diagnosis of endogenous hyperinsulinemia was made and the patient was transferred to the Department of Endocrinology. The patient required a continuous infusion of 10% glucose to maintain low normal serum glucose levels. Fasting, under close medical supervision, was followed by symptomatic and biochemical hypoglycemia within 8-hours from the initiation of the test and during an oral glucose tolerance test (Table 1). As very low serum glucose levels were associated with inappropriately high serum insulin (>6 iu/L,) and detectable C-peptide levels, the diagnosis of endogenous hyperinsulinism was made. As there was no family history of hypercalcemia, pituitary and/or other pancreatic tumours and her serum calcium levels and anterior pituitary hormone levels and pituitary imaging were normal, a sporadic insulinoma was highly suggestive.
Following the biochemical confirmation of hyperinsulinemia an attempt to localize the insulin secreting-tumour was made. Contrast-augmented CT and MR imaging of the pancreas as well as radionuclear imaging with 111In-octreotide failed to localize a pancreatic lesion. An endoscopic ultrasound identified a tumour at the tail of the pancreas, in close proximity to the spleen. A fine needle aspiration (FNA) was performed in order to acquire enough material for cytological analysis using Medi-Glob 22G needles. Cytology followed by immunocytohemistry for chromogranin and insulin suggested a pancreatic insulinoma. The patient remained normoglycemic while receiving treatment with oral diazoxide (150 mg/day). Subsequently, she underwent a laparotomy and the pancreas was exposed. The tumour was not identified and the tail of the pancreas was mobilized without success. IOUS did not locate the tumour. A soft-tissue mass in close contact with the pancreas was removed. We then elected to close the abdomen in order to avoid unnecessary blind distal pancreatectomy and perform a new EUS later. The patient had an uneventful recovery and two weeks later a further EUS was performed. The examination was carried out using Pentax's EUS EG 3630U and Hitachi's console EUB 6000 Victor, which clearly identified a hypoechogenic lesion of 0.98x0.82cm in size, with clear smooth borders, located in-between the body and tail of pancreas, that showed intense and diffuse vascularization in the Doppler signal. Trans-gastric injection of 1cc methylene-blue in the tumour through fine needle was done for tattoing the lesion (Figure 1).

Figure 1. Endoscopic ultrasound revealed the small insulinoma.
Following the successful localization of the lesion the patient was taken to the operating room and a second laparotomy was performed. The anterior surface of the pancreas was explored and a coloured area at the lower surface of the body of the pancreas was clearly visualized (Figure 2). However no tumour was identified either on inspection and/or palpation. Intra-operative ultrasound was performed and detected the tumour at the tattoed-indicated area. The pancreas was then fully mobilized and the tumour was identified at the inferior and posterior aspect of the pancreas, adjacent to the left side of portal vein. The insulinoma was then easily enucleated and the tumour measuring 1.8´1´1cm was removed and submitted to histology. On sectioning, the specimen was whitish with solid, homogeneous appearance. By light microscopy, the neoplasm consisted of solid cellular nests, separated by vascularized connective tissue thin septa (Figure 3).

Figure 2. Intraoperative view of the anterior surface of pancreas. The arrow indicates the tattoed area.
The tumour cells were polyhedral or polar with spheroid nucleus and focally conspicuous nucleolus. Mitoses and apoptosis were scarce. No vascular or nerve invasion was noted. Immunohistochemistry was conclusively positive for chromogranin and insulin and negative for all additional peptides and biogenic amines examined (glucagon, somatostatin, PP, VIP and serotonin). The Ki-67 (clone MIB-1) proliferation maker was positive in a less than 1% of tumour cells (Figure 3, 4). According to these morphological results, the neoplasm was diagnosed as a well-differentiated endocrine tumour producing insulin (insulinoma)3.
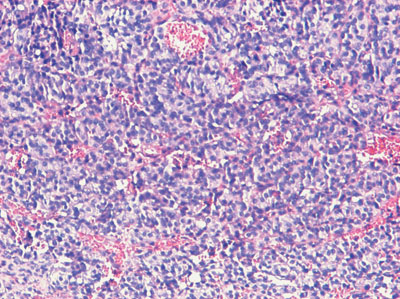
Figure 3. This figure shows a cellular tumour composed of polyhedral cells forming solid nests. The spheroid nuclei show no signs of polymorphism. (Hematoxylin-Eosin stain, original magnification 10X).
The patient had an uneventful post-operative recovery and was discharged 2 weeks later. Currently she remains normoglycemic, 3 years after surgery. A prolonged repeated fasting test (72 hours) was not associated with any hypoglycemia. A repeated MR scan of the abdomen revealed no abnormality in either the pancreas and/or the adrenal glands.
DISCUSSION
The case illustrates the inherent difficulties that may arise in the localization and thus definite treatment of patients with insulinomas4. Insulinomas account for 60% of islet cell tumours (ICT) and are typically hypervascular, solitary small tumours, 90% of which measure less than 2cm and 30% measuring less than 1cm in diameter5. Approximately 10% are multiple, 10% are malignant and 4-7% are associated with MEN I; these tumours are usually multiple and can be malignant in up to 25%5. Almost all insulinomas are located within the pancreas, even though aberrant cases have been described in the duodenum, ileum, lung and cervix5. The tumour is characterized by hypersecretion of insulin and the subsequent development of symptoms of neuroglycopenia and symptoms resulting from the catecholaminergic response, which may not always be present5. As occasionally symptoms are not specific, a broad differential diagnosis is required including a search for sulphonylurea or related drug in the plasma or urine5. Following the biochemical confirmation of an insulinoma, successful excision of the tumour is associated with a normal life expectancy5. It is therefore important to obtain an accurate localization of the tumour.
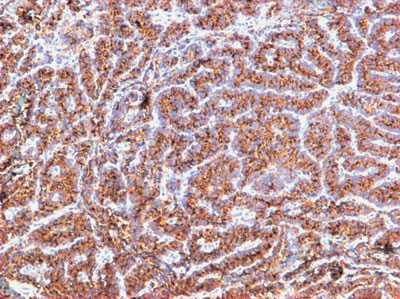
Figure 4. The tumour cells exhibit strong and selective immunoreactivity for insulin (Avidin-Biotin-Peroxidase-Complex technique, original magnification 10´).
Recently, several prospective studies have investigated the relative utility of currently available techniques, and helped to establish a diagnostic work-up on evidence-based information. Because of its high sensitivity and its ability to obtain whole body images, scintigraphy with 111In-octreotide is considered the initial imaging procedure of choice for gastroenteropancreatic tumours (including carcinoids and ICT)5. However, specifically in insulinomas scintigraphy with 111In-octreotide has been shown to be less sensitive than other ICT, as it was also demonstrated in the present case, probably due to the lack of somatostatin receptors type 2 and the small size of the lesions5. EUS allows the positioning of a high frequency (7.5-10 MHz) transducer in close proximity to the pancreas. Using this approach lesions as small as 5 mm as well as tumours located in the bowel can be detected5. Although there is a potential "blind-spot" at the splenic hilum, high sensitivities have been obtained5. A recent single-center prospective study revealed a sensitivity of 93% and a specificity of 95% respectively in localization of intra-pancreatic lesions5. EUS detected all tumours visualized by any other conventional technique questioning the necessity for other imaging modalities. This was clearly evident in our patient in whom EUS successfully identified the lesion; in addition, it aided further to the diagnosis as FNA confirmed the endocrine nature of the tumour. IOUS also allows direct examination of the pancreas using high resolution 7.5-10 MHz transducers. The combination of IOUS and surgical palpation has led to 97% cure rates in patients with benign insulinomas5. However, there are cases, as illustrated by our patient, in which the exact pre-operative localization of the tumour may improve further the diagnostic accuracy of IOUS and thus eliminate the cases of surgical failure. In addition, besides facilitating surgical resection, IOUS can help define the appropriate plane of resection by identifying multiple small tumours, in patients with MEN I5.
The majority of ICT are isodense on unenhanced CT and will not be seen without intravenous contrast enhancement6,7. Dual-face helical CT scan allows multiphase imaging during a single bolus of contrast administration, and can achieve sensitivities in the range 82-92%8,9. A comparative study showed that the sensitivity of T1-weighted MR imaging is equivalent to delayed Portal Venous Phase (PVP) dynamic CT10. Due to the relative rarity of islet cell tumours, it remains difficult to define the best imaging technique, although MRI is probably the investigation of choice in defining hepatic metastases10. MRI is considered the most sensitive technique for demonstrating liver and bone metastases in patients with gastroenteropancreatic (GEP) tumours and is recommended for precise monitoring of response to therapy11. However, both these investigations were negative in our patient necessitating the application of further diagnostic procedures. In cases of small insulinomas not detected with the previously mentioned imaging modalities, invasive procedures may still be necessary to achieve pre-operative localization12. Sensitivities ranging between 77 and 100% have been described for trans-hepatic portal venous sampling (TPVS), but this technique is associated with considerable morbidity12,13. Selective arterial calcium stimulation and hepatic venous sampling (ASVS) using calcium as the insulin secretagogue is a powerful tool for the preoperative localization of occult insulinomas and can also help distinguish the rare forms of non-insulinoma-pancreatogenous-hyperinsulinemia (NIPHS)5. In a recent series of 11 patients a sensitivity of 100% was obtained with this technique, which may also identify rare extra-pancreatic insulin-secreting Neuroendocrine Tumours (NETs), mainly of the liver7,12. Positron emission tomography (PET) using 11C-5-hydroxytryptamine (HTP), due to selective uptake in tumour tissue compared to surrounding tissue, produces very good tumour visibility and it can be used for the examination of both the thorax and abdomen. However, lack of general availability and high cost limits its use14,15. Intra-operative nuclear imaging can be used to help define the exact location of a biochemically proven GEP and aid in its complete resection14.
Conventional imaging studies such as ultrasonography, CT, and MRI fail to reveal the majority of insulinomas16. However they have a role in the evaluation of malignant insulinomas and in the detection of metastases. Portal vein sampling and intra-arterial stimulation of insulin secretion with calcium makes it possible to detect almost all insulinomas but they are invasive and complicated techniques17. IOUS alone identifies approximately 95% of tumours18 but necessitates experience for the surgeon or assistance by a radiologist. Laparoscopic ultrasound as an integral part of laparoscopic procedure has also been suggested in the management of these patients19. However inability to localize the tumour during laparoscopic approach and conversion rate has been reported as high as 30% in a recent multicentre study20.
Preoperative endoscopic ultrasound with fine needle tattooing combined with intraoperative ultrasound can localize the 100% of insulinomas. The technique was first advocated by Gress et al21. It needs experienced endoscopist and surgeon familiar with pancreatic surgery. The overall sensitivity and accuracy of EUS is over 90% for insulinomas22 and EUS-FNT helps even more in localizing the site of the lesion. Our case supports the use of EUS and EUS-FNT as a primary modality in the evaluation, localization and treatment of patients with insulinomas. Nevertheless, CT and MRI scan are still useful in the assessment of malignancy and identification of adjacent lesions.
REFERENCES
1. Hirshberg B, Libutti SK, Alexander HR, et al, 2002 Blind distal pancreatectomy for occult insulinoma, an inadvisable procedure. J Am Coll Surg 194: 761-764.
2. Grant CS, 1998 Insulinoma. Surg Oncol Cl N Am 7:819-844.
3. Heitz PH, Dayal Y, Komminoth P, et al 2004 WHO Classification of Tumours of the Endocrine Organs: Pathology and Genetics of Endocrine Organs. In: DeLellis RA, Heitz P, Lloyd RV, Eng C (eds), IARC Press, Lyon; pp, 10-13.
4. Teale JD, Marks V, 1990 Inappropriately elevated plasma insulin-like growth factor II in relation to suppressed insulin-like growth factor I in the diagnosis of non-islet cell tumour hypoglycaemia. Clin Endocrinol 33: 87-98.
5. Kaltsas GA, Besser GM, Grossman AB, 2004 The diagnosis and medical management of advanced neuroendocrine tumors. Endocr Rev 25: 458-511.
6. Buetow PC, Miller DL, Parrino TV, Buck JL, 1997 Islet cell tumors of the pancreas: clinical, radiologic and pathologic correlation in diagnosis and localization. Radiographics 17: 453-472.
7. King CM, Reznek RH, Dacie JE, Wass JA, 1994 Imaging islet cell tumors. Clin Radiol 49: 295-303.
8. London JF, Shawker TH, Doppman JL, et al, 1991 Zollinger Ellison syndrome: prospective assessment of abdominal US in the localization of gastrinomas. Radiology 178: 763-767.
9. Debray MP, Geoffroy O, Laissy JP, et al, 2001 Imaging appearances of metastases from neuroendocrine tumours of the pancreas. Br J Radiol 74: 1065-1070.
10. Yu F, Venzon DJ, Serrano J, et al, 1999 Prospective study of the clinical course, prognostic factors, causes of death, and survival in patients with long-standing Zollinger-Ellison syndrome. J Clin Oncol 17: 615-630.
11. Shapiro B, Fig LM, 1989 Management of pheochromocytoma. Endocrinol Metab Clin North Am 18: 443-481.
12. Troncone L, Ruffini V, 1997 1311-MIBG therapy of neural crest tumors. Anticancer Res 17: 1823-1831.
13. Erickson D, Kudva YC, Ebersold MJ, et al, 2001 Benign paragaggliomas: clinical presentation and treatment outcomes in 236 patients. J Clin Endocrinol Metab 86: 5210-5216.
14. Mignon M, 2000 Natural history of neuroendocrine enteropancreatic tumors. Digestion 62: 51-58.
15. Hemminki K, Li X, 2001 Incidence trends and risk factors of carcinoid tumors:a nationwide epidemiologic study from Sweden. Cancer 92: 2204-2210.
16. Hiramoto JS, Feldstein VA, LaBerge JM, Norton JA, 2001 Intraoperative ultrasound and preoperative localization detects all occult insulinomas. Arch Surg 136: 1020-1026.
17. Boukhman MP, Karam JM, Shaver J, Siperstein AE, Delorimier AA, Clark OH, 1999 Localization of insulinomas. Arch Surg 134: 818-823.
18. Burns AR, Dackiw AP, 2003 Insulinoma. Curr Treat Options Oncol 4: 309-317.
19. Assalia A, Gagner M, 2004 Laparoscopic pancreatic surgery for islet tumors of the pancreas. World J Surg 28: 1239-1247.
20. Ayav A, Bresler L, Brunaud L, Boissel P, 2004 SFCL (Societe Francaise de Chirurgie Laparoscopique), AFCE (Association Francophone de Chirurgie Endocrinienne). Laparoscopic approach for solitary insulinoma: a multicentre study. Langenbecks Arch Surg (Epub ahead of print).
21. Gress FG, Barawi M, Kim D, Grendell JH, 2002 Preoperative localization of a neuroendocrine tumor of the pancreas with EUS-quided fine needle tattooing. Gastrointest Endosc 55: 594-597.
22. Richards ML, Gauger PG, Thompson NW, Kloos RG, Giordano TJ, 2002 Pitfalls in the surgical treatment of insulinoma. Surgery 132: 1040-1049.
Address correspondence and requests for reprints to:
Dr G Zografos, 10 K. Ourani str, Filothey 152 37 Athens,
Greece, Tel: 2107785031, Fax: 2107706915,
e-mail: gnzografos@yahoo.com
Received 23-12-04, Revised 10-02-05, Accepted 25-02-05